

Did Elon Musk Kill Millions?
No. Just no


Recently, an article in The Argument titled “Elon Musk’s zero accountability life” by Kobe Yank-Jacobs accused Musk and DOGE of helping dismantle USAID and thereby sentencing millions of people to death. Just to be clear, this is not a loose paraphrase of the argument. That is, more or less, the actual claim. He even defends Ro Khanna’s statement that Musk “possibly sentenced” 4.5 million children to death by dismantling USAID. Oh, and just in case the reader somehow missed the point, he adds that at best the toll is around the number killed in the Civil War every year, and at worst Musk is responsible for 14 million deaths.
Now, there are a few different ways one could respond to this.1 The easiest would be to say that foreign aid is often wasteful, corrupt, self-serving, ideologically motivated, and ineffective, which is true enough—but not sufficient. The fact that USAID funded a great deal of nonsense does not mean every part of it was nonsense, and the fact that the people defending USAID are often hysterical does not mean every concern they raise is fake. But, that is also precisely why the death-toll argument deserves more scrutiny, not less. One would think that the question of what happens when a major global-health donor suddenly changes course is important enough to warrant careful and rigorous analysis. Well, this article was anything but that. Repeating “hundreds of thousands” or “millions” of deaths is not a minor exaggeration but an extraordinary accusation, and one that requires extraordinary evidence. If someone wants to accuse a man he dislikes for political reasons of killing on a scale comparable to history’s great catastrophes, then the evidence presented here is not even remotely going to cut it.
Don’t get me wrong, there can be a serious conversation to be had about foreign aid, global health, and what obligations America does or does not have to the rest of the world.2 Unfortunately, before we can have that conversation, we first have to clear away the most theatrical claim in the room: that Musk and DOGE killed, or will kill, millions of people because the people reciting it like a religious chant can’t be bothered to actually check the quality of the evidence behind it.
Before getting into whether the death-toll claim is true, it is worth being clear about what kind of evidence is even being offered. The article’s argument basically rests on three sources: a study published in The Lancet by Cavalcanti et al., henceforth referred to as the Lancet study, estimates from the Center for Global Development, and Impact Counter. These are treated as if they are three independent pillars all pointing toward the same obvious conclusion, even if different in precise magnitude. In reality, they are three different ways of doing the same basic thing: researchers made some bad assumptions, put those assumptions into a model, and the model produced some wildly wrong numbers.
The Lancet study is the high-end one of the three, and the one which estimates that USAID cuts could cause 14 million deaths by 2030, including 4.5 million children under five. Yank-Jacobs leans on this because the number is shocking and because “published in The Lancet” sounds serious to people who do not remember that respectable journals are perfectly capable of publishing bad work when the political mood is right.
To get to the numbers that they did, the Lancet study estimates past associations between USAID spending and mortality, then projects those estimated effects forward under a defunding scenario. That itself is already a difficult task. To get the answer right, the model has to isolate the effect of USAID from everything else affecting mortality in poor countries over the same period: economic growth, sanitation, local health spending, other donors, war, disease-specific innovations, institutional capacity, and the fact that USAID often spends money in places already experiencing health crises. Any correlations that are misattributed as being causal, and the projected death toll can be badly overstated.
The first reason for suspicion is that the results are unusually clean. Across nearly every targeted cause of death, higher USAID spending predicts lower mortality in the expected order, while the placebo outcome—injuries—does not show the same effect. Considering the poor quality of data from these countries, it’s almost miraculous. It’s also exactly the kind of result where robustness matters.
A replication attempt by an independent researcher who goes by “Ralph Balric’s Attourney” (RBA) found that the results are highly sensitive to modeling choices. One major issue is how USAID spending is grouped. The Lancet study’s authors categorize countries into spending bins. However, they appear to bin spending across the entire dataset rather than within each year. But because spending and mortality both change over time, if high-aid observations are disproportionately drawn from later periods, or if mortality was already trending downward, then the spending bins can partly capture time trends rather than the effect of aid. When the spending is grouped by year instead, the all-cause mortality results weakened substantially. In the cause-specific models, some effects remained, but they were smaller and messier. In at least one case, the sign flipped. This raises the possibility of reverse causation: USAID may increase spending in response to a crisis, rather than the spending itself explaining the mortality pattern.
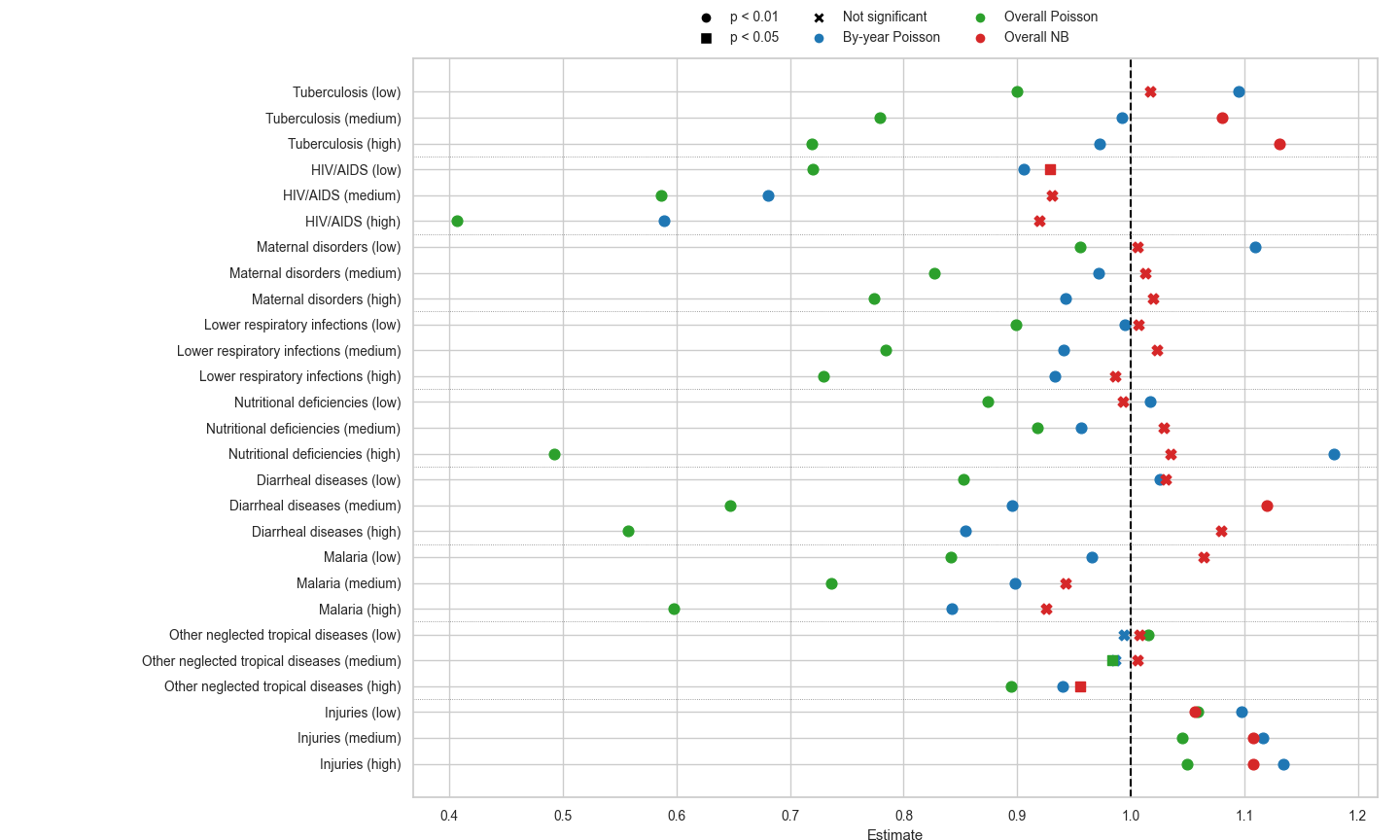
The more serious problem is the use of Poisson regression. To put it simply, a Poisson model assumes that the variation in the number of deaths is relatively well-behaved. But mortality in poor countries is often not well-behaved. Deaths cluster around epidemics, famines, wars, reporting changes, and local crises. When the data vary much more than the model expects, the model can become too confident and make effects look more precise than they really are. A standard alternative is negative binomial regression, which allows for this extra variation. When negative binomial models are used, the results became much weaker. In the HIV/AIDS model, for example, the Poisson specification produced much larger and more statistically impressive effects than the negative binomial specification. The negative binomial version still found some relationship, but nothing like the dramatic effect size needed to justify the article’s rhetoric.
The Lancet study’s authors knew this was a problem, so they did try a negative binomial version. However, they rejected it because their Poisson model had better AIC/BIC scores. In theory, those scores tell you which model fits better after penalizing unnecessary complexity. The problem is that this comparison only works when the scores are actually comparable. In this case, they are very much not. The Poisson and negative binomial models were not being evaluated with the same underlying likelihood setup, so the AIC/BIC numbers were not measuring the same thing.
It’s evident that this matters tremendously, because the difference was not small. In the Lancet study’s supplement, the Poisson and negative binomial information criteria differed by orders of magnitude, roughly tens of thousands versus millions. Rather than treating this as the Poisson model fitting better, it should have been treated as a sign that the comparison was broken. The better question was whether the mortality data were over-dispersed. On the HIV/AIDS data, RBA reported a massive over-dispersion test result, which is exactly the condition under which Poisson becomes inappropriate and negative binomial becomes the more natural choice. Once that model is used, the effects become much smaller, and given that the projected death toll depends on the estimated effect sizes, the 14 million figure is not a reliable “high-end estimate” in the slightest bit.
This is why “peer-reviewed” is not an answer. Peer review does not turn fragile models into facts.3 Journals publish bad studies all the time, especially when a paper flatters the political priors of the class of people likely to review it, promote it, and write about it afterward.
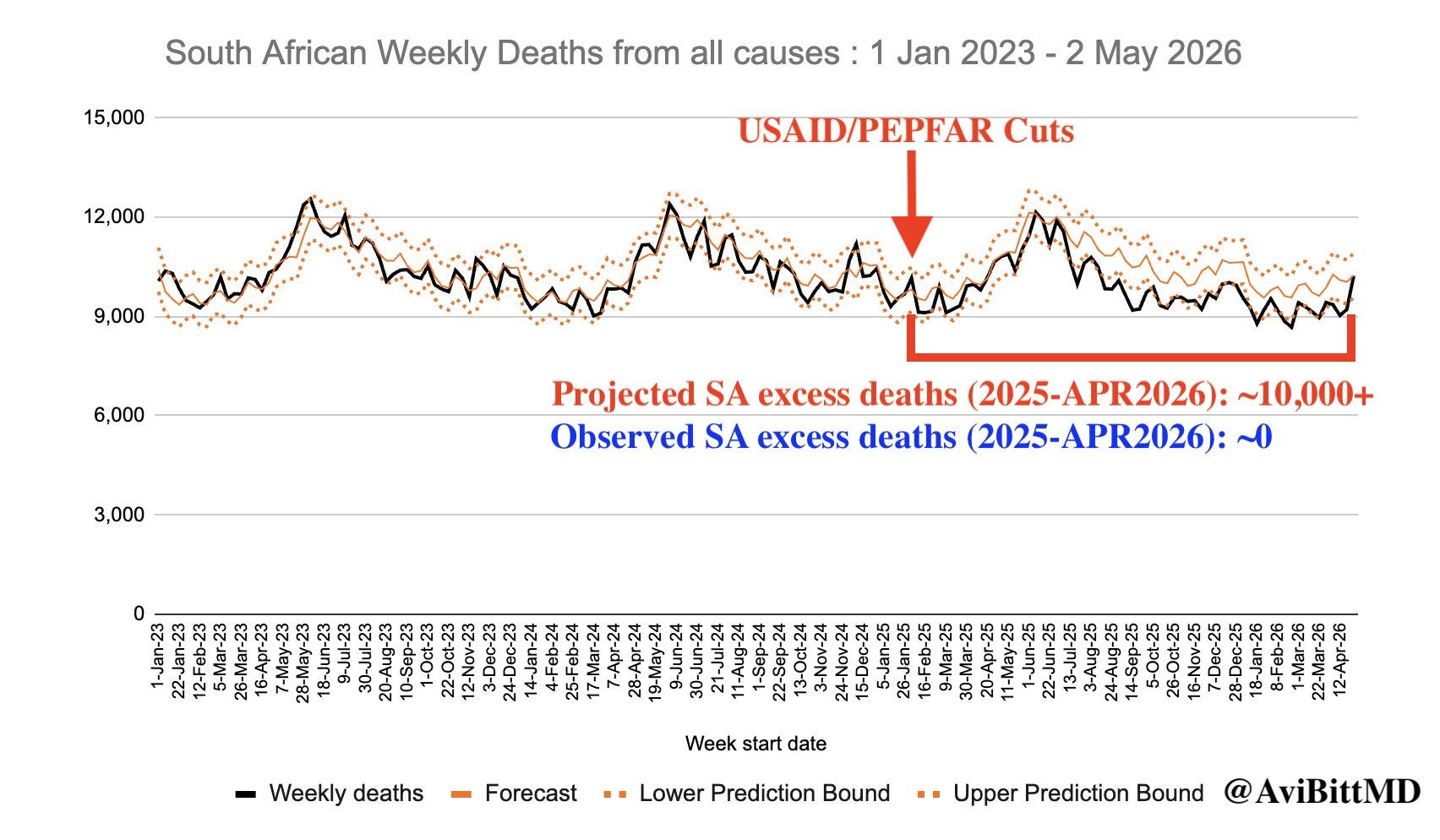
Meanwhile, provisional mortality data from Egypt outright failed to show the predicted spike. Egypt is not the perfect test case, but it did have substantial USAID exposure under the Lancet study’s spending categories. The first available post-cut mortality datum showed fewer deaths in May 2025 than in May 2024, with levels broadly comparable to 2022 and 2023. While this does not settle the global question, if the claim is that hundreds of thousands have already died, the first available mortality datapoint from a USAID-exposed lower-middle-income country showing no excess mortality should at least make people pause. The same is true with South Africa, which is among the largest recipients of USAID programs:4
The article tries to dispose of one sanity-check critique of the Lancet study from Aaron Brown in Reason Magazine. Brown noted that, if you hold the world’s 2001 death rate constant and compare it with actual deaths from 2001 to 2021, you get about 79 million fewer deaths. The Lancet study claims USAID saved 91.8 million lives over that same period. On its face, then, the study seems to credit USAID with more than the entire global mortality improvement, plus another 11 million “phantom lives”. Yank-Jacobs responds that this is too simple because the global population grew and aged after 2001. In his telling, merely holding the 2001 death rate constant would itself have been a kind of achievement, so the Lancet study’s estimate is not disproven just because it exceeds that naïve 79 million figure.
But this does not rescue the Lancet study’s estimate. While Yank-Jacobs is correct that using a flat 2001 death-rate baseline as a no-USAID counterfactual is not sensible, the actual reason why is because that’s already giving USAID too much credit. Death rates had been falling, and life expectancy had been rising, long before 2001. In Africa, the improvement in life expectancy and age-specific mortality was part of a broad post-1950 trend (astute readers may have noticed that this trend predates the creation of USAID). In fact, it’s hard to see from the broader picture over a longer time period if USAID was responsible for really anything. Here’s some visuals from Our World in Data:




If the total improvement relative to a flat 2001 baseline is 79 million, and USAID alone supposedly saved 91.8 million, then the model is already asking us to believe something very large. Of course, 79 million is already too many. Moreover, if much of the observed mortality decline happened in countries with little USAID exposure, while the highest-USAID countries did not show comparable aggregate improvement, the burden becomes even heavier. The Lancet study’s model appears to be claiming ownership over a mortality decline that was already underway, had many causes, and was often largest in places where USAID could not plausibly have been the main driver. This latter point that was made by Brown in the Reason Magazine article is not addressed by Yank-Jacobs at all.
After the article treats the Lancet study as the high-end estimate, it then turns to the Center for Global Development and Impact Counter as more conservative confirmations of the same basic story. This appears to be a tactic employed by Yank-Jacobs so that the article’s fallback position is that even if the Lancet study’s estimates are too high, the lower estimates are still large enough to imply a catastrophe.
CGD estimates that the USAID cuts could produce between 670,000 and 1.6 million additional deaths annually. Its method is simple: estimate how many lives are supposedly saved per dollar of U.S. foreign aid, estimate how many dollars were cut, and multiply the two. The formula is literally:
Lives lost = (lives saved per dollar by US foreign aid) × (dollars cut in 2025)
But this model is clearly way too simplistic. CGD is fairly open about this, describing its lives-saved-per-dollar estimates as “ballpark estimates”. While a model can be used to estimate the amount of aid used to save X many lives on average, it cannot automatically tell you how many people actually died. Why not? Because it ignores the basic fact that people and governments respond to change.
Models like CGD’s implicitly assume a static world. USAID funding disappears, programs disappear, patients lose treatment, and deaths follow suit. That is how you get large numbers quickly. It also has no bearing on actual reality. Here’s a useful comparison: abortion. If there are 1 million abortions in a year, one cannot simply say that banning abortion would produce 1 million additional births. A share of those pregnancies would be carried to term, but people also change their behavior: contraception, sex, marriage timing, birth planning, illegal abortion, travel, and so on. This explains why studies on the effects of abortion restrictions find far more modest boosts to fertility than what would simply be predicted by the existing number of cases each year. In the real world, humans react.
A subsidy lowers the cost of staying alive. Removing it can, in theory, be harmful. For instance, it can make medicine harder to obtain and increase the chance of missed treatment, which forces people into worse tradeoffs and thereby raising the probability of death. At the same time, however, “higher risk” is not the same thing as “automatic death”. People may find workarounds, like cheaper suppliers, switching clinics, relying on family networks, receiving help from local charities, or make sacrifices elsewhere in order to preserve the treatment that matters most. Governments also learn to adjust spending accordingly when aid is cut.
Once incentives change, institutions and individuals respond. The question is how much harm remains after those responses, not how many deaths a static model produces before anyone is allowed to adapt. ODI reported that African governments responded “proactively” to disruptions in U.S. aid, especially in health. Many governments increased domestic health allocations or created new institutional arrangements aimed at self-reliance. Nigeria approved an additional $200 million for its health sector to offset the U.S. aid shortfall, with much of the money intended for vaccines and epidemic disease treatment. Ghana and Ethiopia also shifted domestic resources in response to the shock. Examples like these are exactly what a static death counter cannot see.
Impact Counter has a different problem. Its presentation makes it look like a death counter, but its own site describes the dashboard as a projection of the one-year human impact of funding changes, frozen at the one-year horizon from when the cuts began. Yank-Jacobs cites Brooke Nichols’s modeling tracker for roughly 260,000 adult deaths and over 500,000 child deaths at the one-year mark, then says that simply extending the trend would produce at least 2.5 million deaths by 2030.
The PEPFAR tracker gives a useful example of how the method works. PEPFAR is the President’s Emergency Plan for AIDS Relief, America’s main global HIV/AIDS program. For adult HIV deaths, Impact Counter assumes a complete disruption over a three-month period, averages results across existing mathematical models of HIV service interruption, and then attributes 47% of the resulting deaths to PEPFAR because PEPFAR funds roughly 47% of HIV programs in those sub-Saharan African countries. That produces an estimate of about 159,000 adult deaths over one year from the PEPFAR disruption alone.
For child HIV deaths, Impact Counter starts with UNAIDS estimates of women using services that prevent mothers from transmitting HIV to their children during pregnancy, birth, or breastfeeding. It assumes transmission rises from about 1% with treatment to around 40% without it, applies PEPFAR’s funding share, and then estimates deaths among infected children.
The tuberculosis tracker works similarly. Tuberculosis is a bacterial disease, usually affecting the lungs, that is treatable but can be deadly when diagnosis and treatment break down. Impact Counter models funding discontinuation across 26 high-burden countries and presents different scenarios depending on whether funding resumes within three months, within a year, or never resumes. Under the one-year scenario where funding resumes within a year, it estimates about 55,000 additional tuberculosis deaths over one year. Under the “never resumed” scenario, the projected 2025–2030 death toll becomes much larger.
The good thing about these numbers is that these are scenarios, not observations, meaning that they can be falsified by looking at the actual outcomes. If the funding disruption had produced anything like the mass treatment collapse implied by the worst rhetoric, we should see it in the 2025 numbers. Instead, UNAIDS—the United Nations program on HIV/AIDS—reported continued improvement on the most important topline measures.5 New infections declined slightly from 2024 to 2025, while AIDS-related deaths fell from 600,000 to 570,000 during this time, and the number of people on antiretroviral treatment rose to 32.1 million by the end of 2025. It is clear then that Impact Counter’s HIV estimates are driven by faulty assumptions about treatment interruption. The actual data shows treatment coverage rising, not collapsing.

The main weakness was prevention. UNAIDS reported a 38% decline in PrEP access across 62 countries. PrEP, or pre-exposure prophylaxis, is preventive medication taken by people who do not have HIV but are at risk of infection. HIV testing also fell by 22% in some high-burden countries. While that could be a potential issue, even here the story is not simply catastrophe. Prevention declines do not instantly translate into observed deaths, and the treatment side—the part most directly tied to near-term mortality—continued improving. On top of that, HIV prevention is entering a different technological environment. The U.S. and the Global Fund expanded access to lenacapavir, a twice-yearly injectable HIV-prevention drug, aiming to reach an additional 1 million people over three years and 3 million people through 2028. Lenacapavir has shown near-100% effectiveness in clinical trials, and rollout has already begun in several African countries. Again, the real world did what static death counters do not model. The most valuable services were prioritized, local systems adapted, and treatment continued expanding. Prevention took a hit, but new tools and replacement efforts are already changing the trajectory.
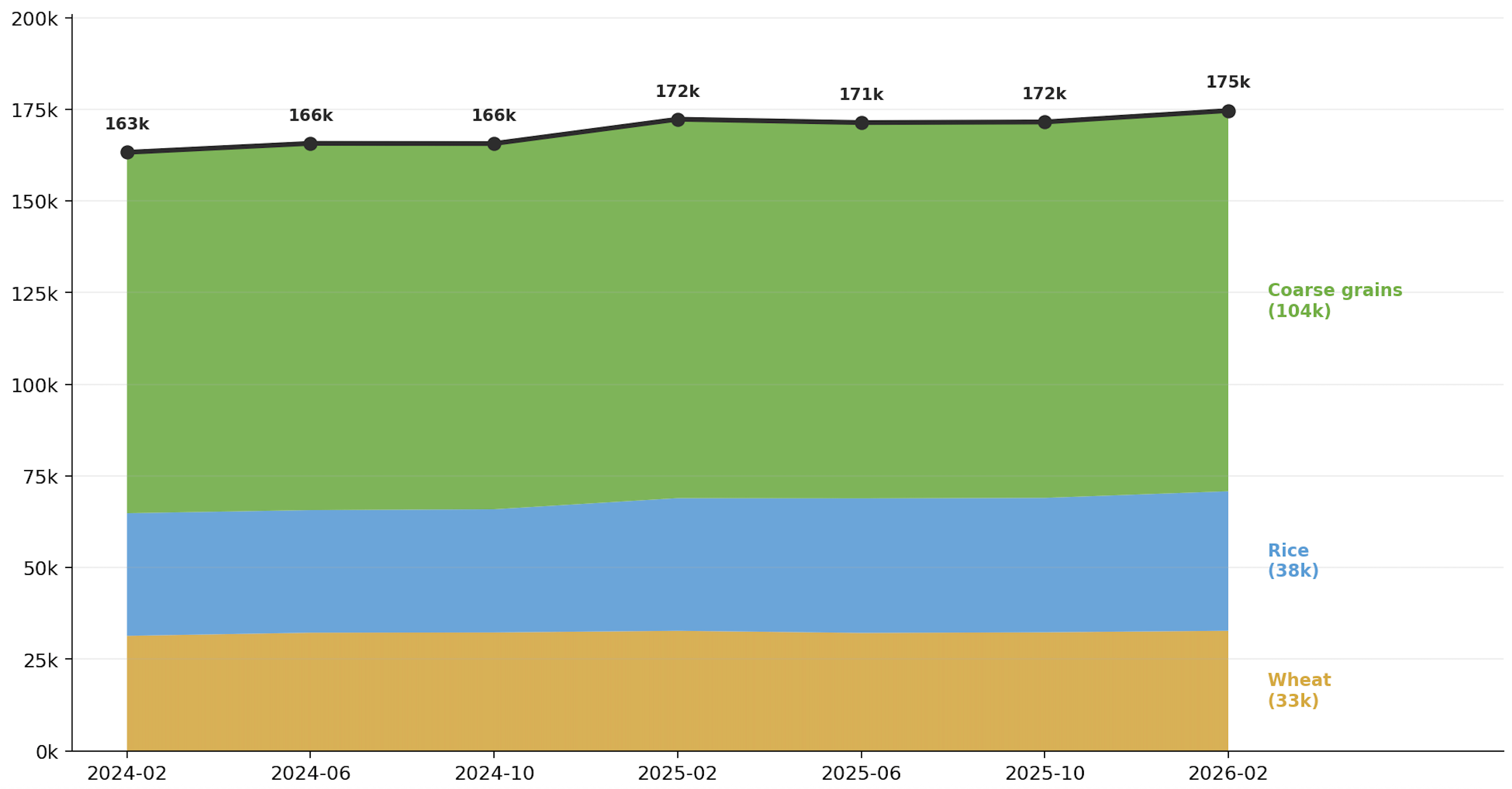
Other sanity checks point in the same direction. If hundreds of thousands of people had already died from a generalized aid-withdrawal catastrophe, one would expect some broad evidence of crisis. Yet food-use data from the Food and Agriculture Organization do not show a collapse in Sub-Saharan Africa after USAID was rolled up. The trend remains broadly stable and rising slightly. While that does not rule out local hardship, it does make the famine-style rhetoric much harder to take seriously.
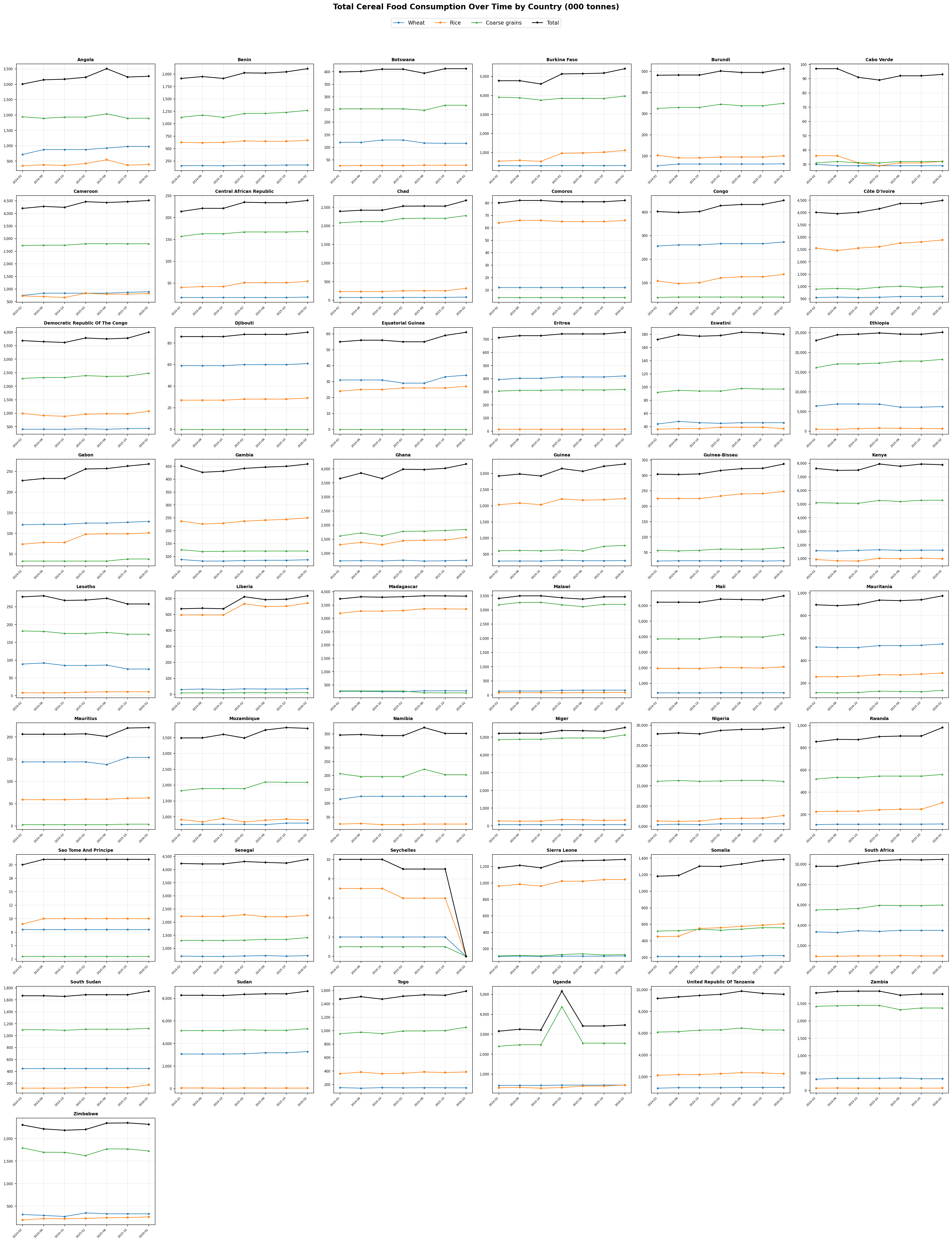
Disaggregating the data, it would appear that, with a few exceptions, the USAID cuts do not seem to have impacted food consumption in most Sub-Saharan African countries:
Another issue is a conceptual one: what we do actually mean when we say “lives saved”? In many of these models, a “life saved” really means a death averted within a particular time window, rather than saving an entire lifetime. Preventing the death of a child who then lives another seventy years and delaying the death of a very sick adult by one year may both enter the tally as one “life saved”. For technical public-health purposes, this could plausibly be justified as legitimate. In political rhetoric though, it makes the effect sound much larger and more permanent than the underlying measure may justify. This becomes even more important for programs that must be repeated every year. If an intervention prevents the same person from dying this year, and then must do the same thing again next year, each annual counterfactual can be counted as another death averted. As a result, headline numbers can easily give less attentive readers the impression of unique, full lives permanently rescued when the underlying metric may be closer to temporary mortality deferral under continuing support.
There’s a broader question behind all of this: does foreign aid, in practice, even produce the kind of huge population-health effects these models assume? The evidence is not very flattering. Toseef et al. (2019) looked at 90 developing countries from 2001 to 2015 and tested whether total foreign aid and health-sector aid improved infant mortality, life expectancy, death rates, measles immunization, and DPT immunization. This is important because they did not only look at health aid. They also used total aid, which gives indirect pathways—education, infrastructure, water, sanitation, and so on—a chance to show up.
The result was mostly null. Aid showed a statistically significant relationship with life expectancy, but the effect was tiny. In their main models, a 1% increase in total aid was associated with only a 0.004% increase in life expectancy. Health aid performed similarly. Their Generalized Method of Moments (GMM) robustness checks found no impact of aid on any health outcome. It seems that once you look across countries and over time, the simple story that foreign aid reliably converts into large health gains becomes much harder to defend.
So, let’s take a step back and remind ourselves what this post is responding to. The claim is that Musk and DOGE killed, or will kill, millions of people; that the rollback of USAID can be translated into one of the great death tolls of the modern era; that projected deaths from unreliable models should be treated as essentially confirmed casualties. Nope. Sorry, but that’s not how this works. If you want to say certain programs should have been preserved, make that argument. If you want to say the cuts were too abrupt, make that argument. But if you want to accuse someone you dislike politically of killing on the scale of the Civil War every single year, then you do not get to wave around fragile models, online counters, and gross estimates that explicitly do not account for adaptation, and then act as if the matter is settled—especially not when the actual evidence that arrived afterward failed to bear out the catastrophe they predicted.
As the article is paywalled, I can only respond to the free and public portion, though I doubt there’s much more additional substance beyond the paywall.
And, as I don’t believe the United States has any moral obligation to help prop up dysfunctional societies that practice things like dry sex, “virgin cleansing”, and mass rape—especially not when the same people who insist we have to bear this responsibility to begin with are also usually of the belief that America is a morally decrepit empire that intentionally sabotaged the development of the Third World—I am the most objective and fair writer on this topic, since I have no motivations to care about whether or not the numbers are true.
One possible reply is that the mortality data are simply lagging behind the policy shock. That would be more persuasive if the models had mostly projected deaths far into the future. But the more detailed HIV projections did not do that. Even when the studies covered five- or ten-year windows, the deaths were not expected to arrive only years later. In models that break the estimates down by year, a large share of the projected deaths was expected early, with peak death rates generally appearing in 2025 or 2026. If those projections were roughly right, the early mortality signal should already be visible.
South Africa reflects part of a broader problems with the post-hoc excuses. Before the data came out, South Africa was treated as part of the catastrophe. Many models projected large numbers of excess HIV deaths because USAID had been cut, and the implication was clear: South Africa was dependent on that funding, and cutting it would be deadly. But once the provisional mortality data failed to show the predicted spike, the explanation suddenly changed. Now South Africa is too wealthy, too institutionally capable, too responsive, or too resilient to be a fair test case. And even if that were true, that is still a concession that the model missed the things that mattered.
If South Africa adapted because its government, clinics, and health system were able to preserve core services, then it’s obviously the case that the assumptions baked into the models were wrong. If local actors redirected resources, prioritized treatment, and prevented the collapse, then these models well-overstated the harm by failing to account for adaptation. And if South Africa was always capable of doing that, then one has to ask an even more awkward question: how much of this foreign aid was actually indispensable in the first place? The defenders of USAID do not get to predict catastrophe, fail to find said catastrophe, and then declare the absence of catastrophe irrelevant because the country turned out to be more competent than their models allowed.
When I did the replication work cited here almost a year ago, I was completely stunned The Lancet paper got literally no critical attention. Lone voice in the wilderness.
Thanks for the work, but I think surrendering the frame is the fundamental problem.
1) "Killing" means you harmed people. At best Musk refused to harm people (US taxpayers) to try and save third worlders from their own dysfunction.
That certainly isn't "killing". And if it is, basically every first worlder that isn't going full EA donating 90% of your income is a killer.
2) Let's say all these third worlders did die. Is that a bad thing?
These African hellholes are all above their malthusian carrying capacity.
Without foreign aid, they will die. With foreign aid they will multiply and require exponentially more foreign aid, until eventually we can't provide it.
Worst of all, all these excess people might move to the west, where they will gain access to the welfare state (100x burden) and influence our politics and society (perhaps turning us into third world hell holes and destroying global society).
Meanwhile, all human advancement comes from smart people reinvesting into economic growth. It's obvious that using USAID funds to fund growth will do more for future people than USAID to Africans today by a factor of like 1000000000x. So any EA case that cares about the future still says cutting aid is good.